Anti-β2-Glycoprotein I [Anti-β2GPI] assays
Anti-Domain I assays
Introduction
The laboratory diagnosis of antiphospholipid antibodies is based upon the use of phospholipid-dependent tests. These tests include screening for the presence of a Lupus Anticoagulant [covered elsewhere] and screening for both Anticardiolipin [aCL] and Anti-β2Glycoprotein I [anti-β2GPI] antibodies.
β2Glycoprotein I (β2GPI) - also known as Apolipoprotein H - is a 326 amino acid, 50-kDa phospholipid-binding protein, present in plasma at a concentration of ~200 mg/ml. It has a number of roles in haemostasis, fibrinolysis, angiogenesis and atherosclerosis - see Ref 8.
β2GPI has been described as a natural anticoagulant that inhibits the intrinsic coagulation pathway, Prothrombinase activity and ADP-dependent platelet aggregation.
β2GPI has five domains [D1 - D5] - see below...
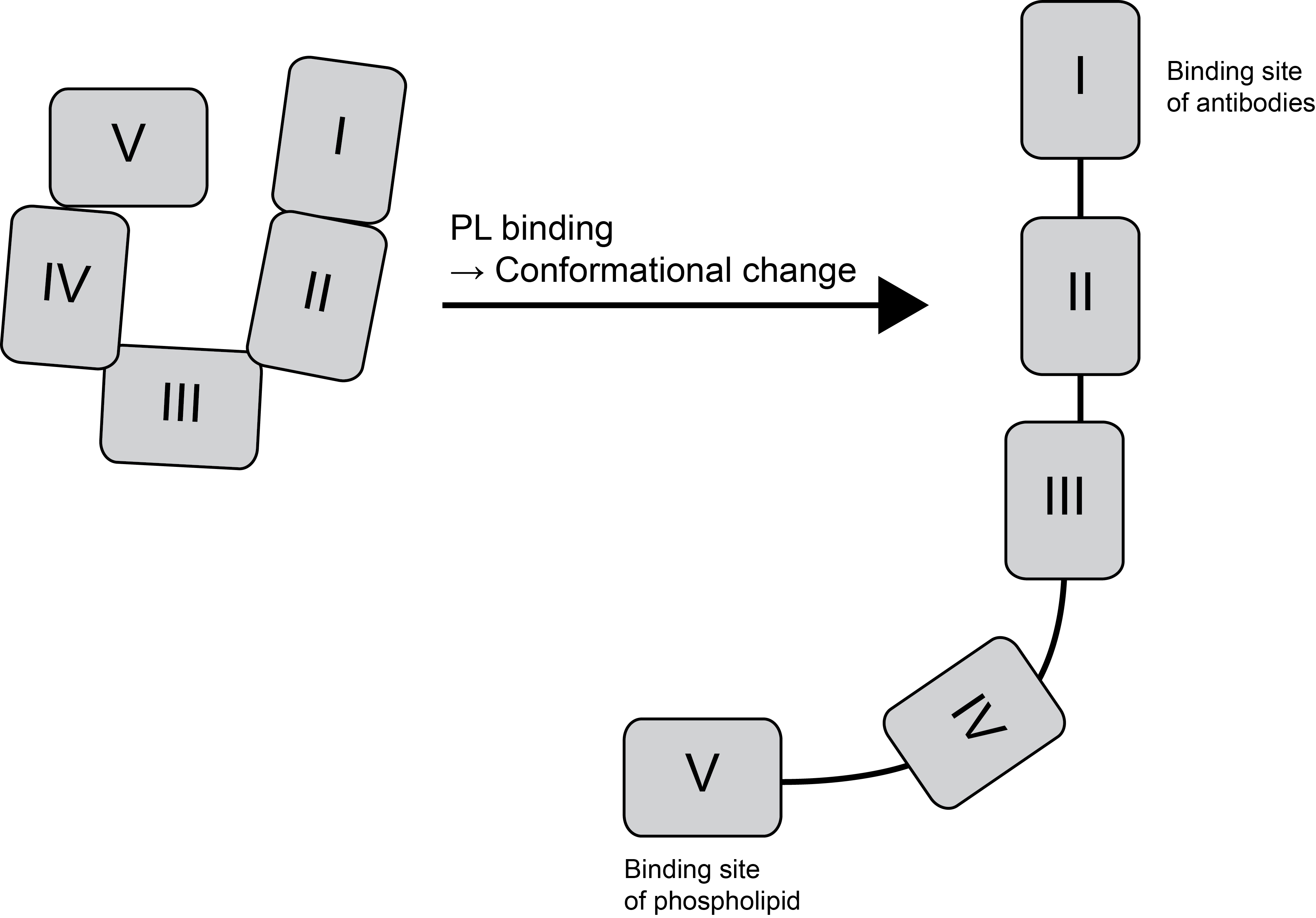
..with significant homology between the five domains. Domain 1, the N-terminal domain, is the main antigenic site for autoantibodies and multiple studies have shown that antibodies to Domain I] are most closely linked to the development of thrombosis. Domain V has an extended C-terminal loop region and is highly flexible. Domain V is involved in the interaction with phospholipid. Circulating β2GPI has a circular shape with Domain I interacting with Domain V and this conformational structure sterically inhibits binding to Phospholipid. High affinity binding to PL results in a conformation change in the structure of β2GPI .
Cardiolipin is found almost exclusively in the inner mitochondrial membrane where it performs an essential role in regulating the enzymes involved in mitochondrial energy metabolism. The term 'cardiolipin' originates from the fact that it was first isolated from bovine heart in the early 1940s and formed the basis of the Wasserman test for syphilis. It was originally thought that APLs were autoantibodies directed against anionic phospholipids and which disrupted the assembly of the Tenase and Prothrombinase complexes. However, it was subsequently shown that these were antibodies directed against phospholipid-binding proteins - β2GPI and occasionally Prothrombin.
In the Antiphospholipid Syndrome [APS] the major target of antiphospholipid antibodies [APL] is β2GPI. Binding of β2GPI to anionic surfaces converts the protein from a structurally 'closed' form that is non-immunogenic to a structurally 'open' form that is immunogenic allowing, potentially, the formation of anti-β2GPI antibodies. The subset of antibodies that bind β2GPI correlate strongly with the thrombotic complications of APS and more recent studies have shown that anti-DI [anti-Domain I antibody] positivity is an independent risk factor for thrombosis in APS.
Principles & Methodology
A number of approaches are available for the detection of aCL and anti-β2GPI antibodies and although commonly detected by ELISA assays, a number of automated methodologies employing e.g. magnetic microparticles and microspheres and various detection systems have become available.
The antigen used in the anti-β2GPI ELISA is recombinant human β2-GPI and there are slight epitope differences between human and bovine β2-GPI. For these reasons it is possible to find individuals who have a negative Anticardiolipin antibody screen but who are positive in an anti-β2-GPI ELISA.
A continuing problem with both assays is the large variability in results and the ISTH has published guidance on these assays in an attempt to minimise the variability in results - see Ref 10.
Interpretation
The three characteristics of relevance for antiphospholipid antibodies are the target antigen, the isotype and the titre.
To be significant the antiphospholipid antibodies must be:
a) Directed against either cardiolipin (aCL) or β2-glycoprotein-I (anti-β2GPI)
b) IgG and/or IgM
c) Present in medium-high titre (i.e. >40 GPLU [IgG] or MPLU [IgM] for aCL or >99th percentile for either aCL or anti-β2GPI.
Reference Ranges
To be significant the antiphospholipid antibodies must be:
a) Directed against either cardiolipin (aCL) or β2-glycoprotein-I (anti-β2GPI)
b) IgG and/or IgM
c) Present in medium-high titre :
>40 GPLU [IgG] or MPLU [IgM] for aCL
>99th percentile for either aCL or anti-β2GPI.
What Test Next
If a positive aCL or Anti-β2-GPI result is found [see above] it is important that it is repeated after 12 weeks to establish if the test is persistently positive or only transient The latter tend to have a low risk of clinical problems associated with them. it is also important to establish if there is any cause for the development of the antibodies and this includes:
i. Systemic autoimmune disorders such as SLE
ii. Infections
iii. Malignancies
iv. Non-malignant Haematological disorders
v. Drugs
vi. Miscellaneous
Anti-Domain I Tests
The Domain I of β2GPI appears to be the main epitope targeted by antibodies reacting against β2GPI. Domain I is a cryptic epitope, becoming available for auto-antibody binding when β2GPI opens from a circular to a linear or fish-hook configuration. Antibodies to Domain A appear to target a positively charged epitope, spanning amino acids 39/40-43. Conformational changes in the structure of β2GPI allows exposure of this epitope in domain I and so enables anti-β2GPI antibodies to interact with the epitope.
Some patients with APS develop antibodies directed against other β2GPI epitopes suggesting that other anti-β2GPI antibody subsets are clinically important. Some data has shown that anti-Domain IV/V antibodies are associated with non-thrombotic autoimmune disorders.
A number of methods for the detection of anti-β2GPI Domain I antibodies have been published - see Kelchtermans et al 2018.