Introduction
The following table provides a summary of the results obtained using the PT, APTT, Fibrinogen and Thrombin Time in various disorders.
| Platelet Count | PT | APTT | TT | Fibrinogen | Interpretation |
|---|---|---|---|---|---|
| Normal | Normal | Normal | Normal | Normal | Normal profile Factor XIII deficiency Mild VWD Qualitative platelet disorder Connective tissue problem e.g. Ehlers Danlos Mild coagulation factor deficiency |
| Normal | ↑ | Normal | Normal | Normal | FVII deficiency |
| Normal | Normal | ↑ | Normal | Normal | FVIII, FIX, FXI or FXII deficiency VWD - if the FVIII level is reduced Lupus anticoagulant - occasionally a very strong lupus anticoagulant or a lupus anticoagulant that has anti-Prothrombin [Anti-II] activity can result in a prolonged PT. Similarly a lupus anticoagulant can also be associated with thrombocytopaenia.] Other contact factor deficiency e.g. HMWK, Pre-Kallakrein |
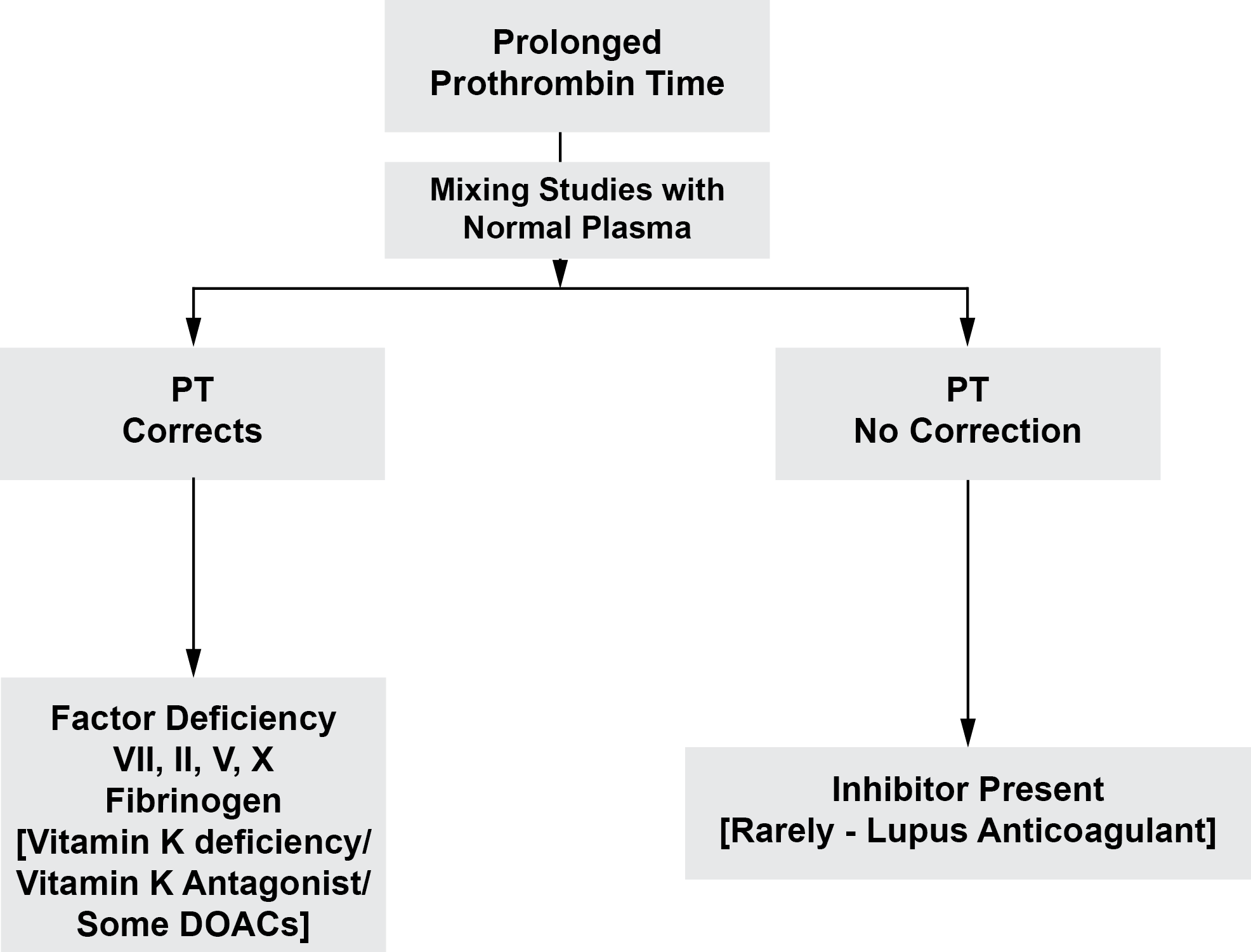
| Normal | ↑ | ↑ | Normal | Normal | 'Common pathway' deficiency i.e. FII, FV or FX deficiency Multiple clotting factor deficiencies e.g. combined FV and FVIII deficiency Warfarin or vitamin K antagonist Vitamin K deficiency or a mutation within one of the genes encoding key enzymes involved in VK metabolism. Occasionally a very strong Lupus anticoagulant can cause these findings but it is unusual to see a prolongation of the PT with a LA due to the high concentration of PL used in the PT test. |
| ↓ | ↑ | ↑ | ↑ | ↓ | DIC Massive transfusion Liver disease |
| ↓ | Normal | Normal | Normal | Normal | Primary platelet problem e.g. ITP. The Mean Platelet Volume [MPV] can be helpful in establishing the causes of thrombocytopaenia. A raised MPV is often associated with increased peripheral destruction e.g. ITP - whereas a reduced MPV is often seen in association with bone marrow failure. A raised MPV can also be found in a number of inherited qualitative platelet disorders. Changes in the MPV are also seen in patients with various inherited platelet disorders e.g. Wiskott Aldrich syndrome in which the MPV is significantly decreased. |
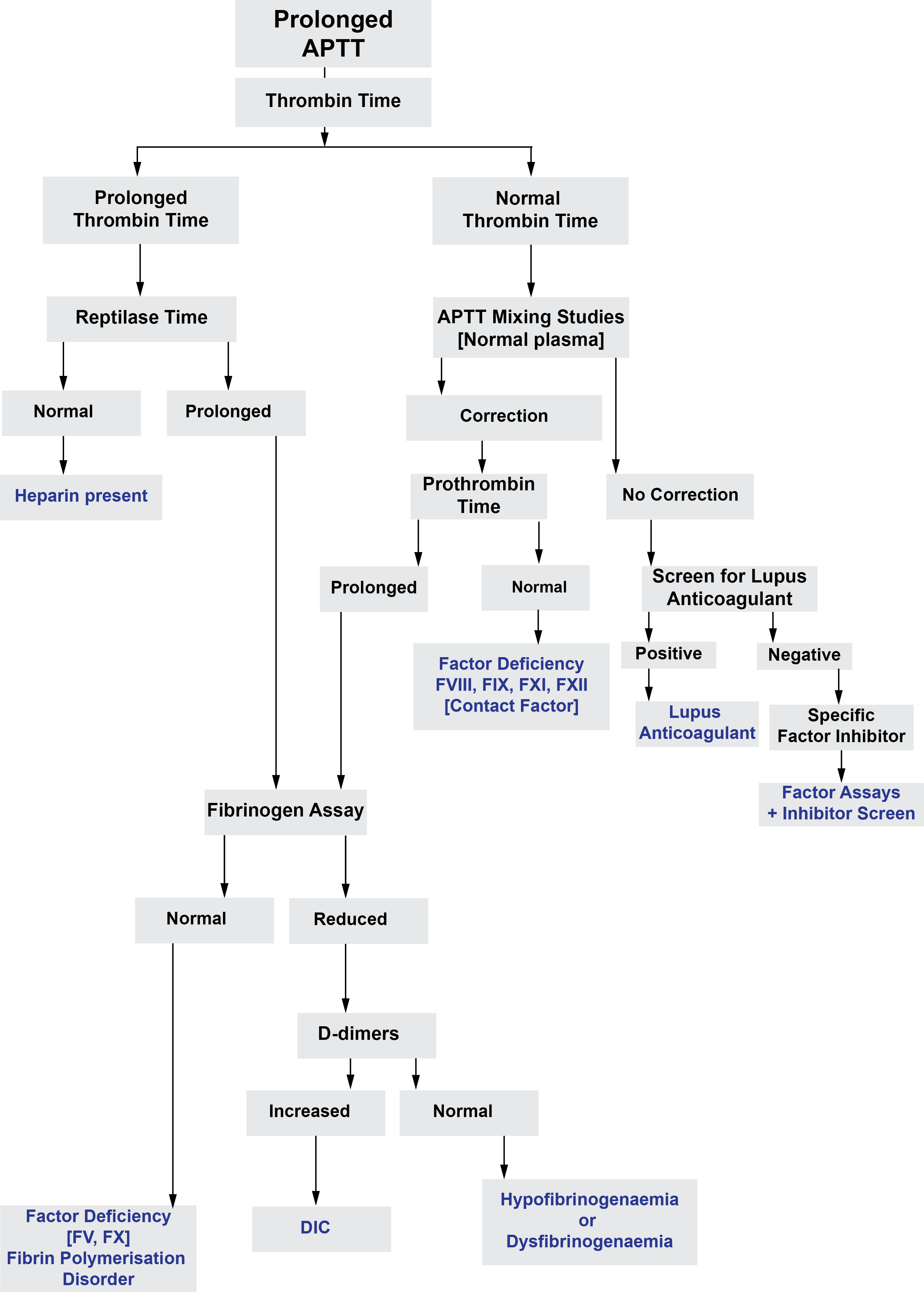
The two diagrams below summarise the investigation of a prolonged PT or APTT...
The following table summarises the results of screening tests in patients who may be taking an anticoagulant.
See also the section on Direct Oral Anticoagulants [DOACs] under 'Useful Information' for further information on the effects of anticoagulants including the DOACs on a number of clotting tests.
| Drug | PT | APTT | TT | Fibrinogen | Comments |
|---|---|---|---|---|---|
| Warfarin and similar Vitamin K antagonists | ↑ | ↑/N | No significant effect | No effect | The APTT may be prolonged in patients whose INR on Warfarin is significantly prolonged |
| Unfractionated Heparin | ↑ | ↑ | ↑ | No effect | |
| Low Molecular Weight Heparin | No effect | No effect | May be prolonged | No effect | |
| Dabigatran | ↑ - test has low sensitivity and results vary with thromboplastin used in the test | ↑ in a curvilinear manner but vary with reagents used in the test | ↑ | No effect or factiously low | A normal TT excludes significant Dabigatran levels |
| Apixaban | ↑ | ↑ | No significant effect | No significant effect | |
| Edoxaban | ↑ | ↑ | No significant effect | No significant effect | |
| Rivaroxaban | ↑ - results vary with the specific thromboplastin used in the test | No significant effect | No significant effect | ||
| Fondaparinux | No effect | No clinically significant effect | No significant effect | No significant effect |
The BSH has published guidelines on the assessment and management of bleeding risk prior to invasive procedures - see References for further information.
Click HERE to return to the top of the page.