Euglobulin Clot Lysis Time [ECLT]
Introduction
The Euglobulin Clot Lysis Time [ECLT] is a test that reflects the overall fibrinolytic activity of plasma. In many cases (perhaps all) it has now been replaced by specific functional and immunological assays. The TEG/ROTEM often serves to monitor fibrinolysis and is a considerably more rapid test to perform than the manual ECLT.
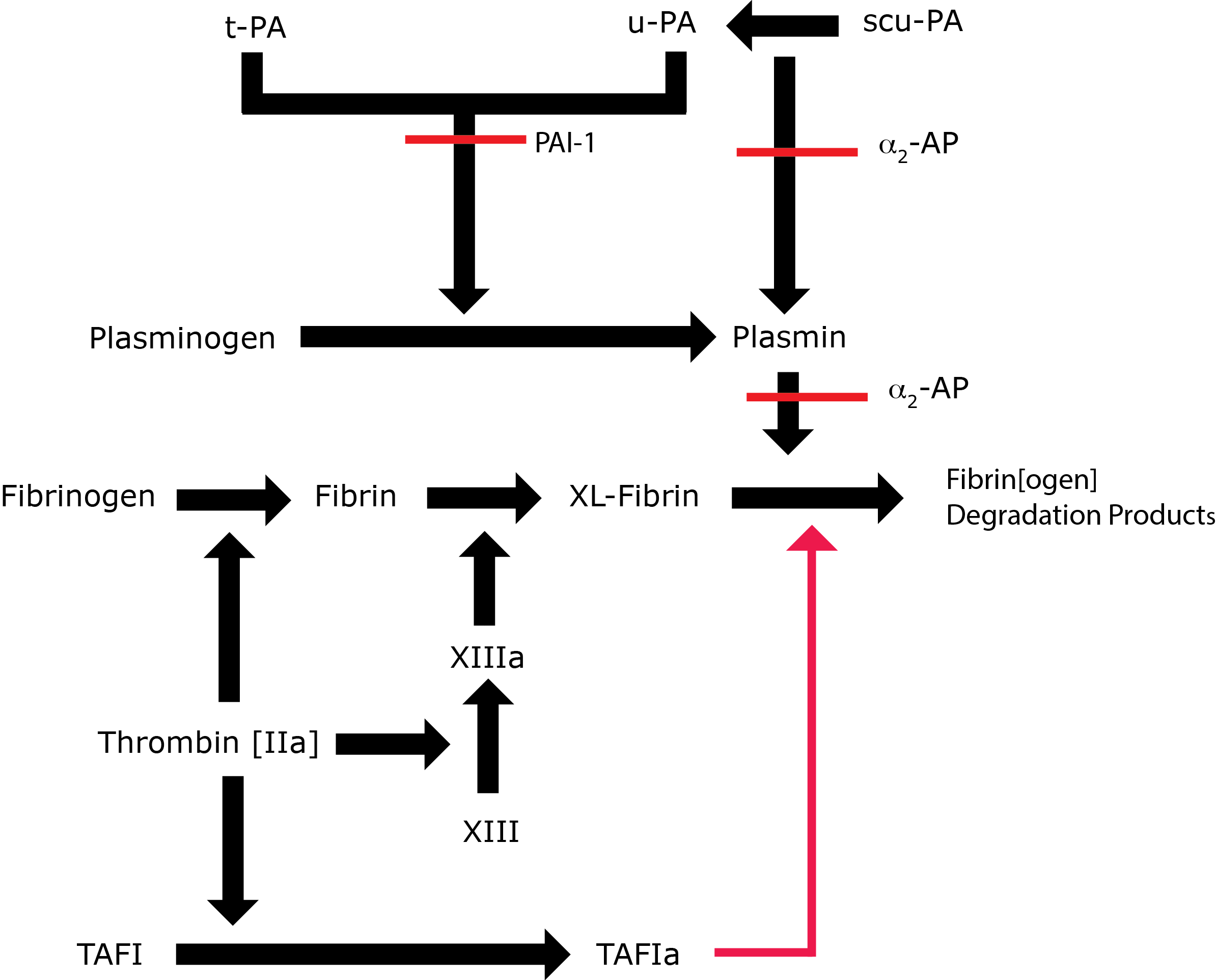
Key: t-PA - Tissue Plasminogen Activator; u-PA - Urokinase-type Plasminogen Activator; XL-Fibrin - cross-linked fibrin; TAFI - Thrombin Activatable Fibrinolytic Inhibitor; TAFIa - Activated Thrombin Activatable Fibrinolytic Inhibitor; α2-AP - Alpha-2-antiplasmin [Alpha2-Plasmin Inhibitor]; scu-PA - single chain Urokinase-type Plasminogen Activator. A red line indicates an inhibitory pathway.
Principles & Method
Venous blood is collected into chilled tubes containing trisodium citrate as an anticoagulant and placed on ice. The sample is then centrifuged at 4°C, the plasma sample is collected, diluted with Acetic acid and incubated on ice for 15 minutes. A precipitate forms [the Euglobulin fraction of plasma] which contains Plasminogen, Plasminogen activators [primarily t-PA] and Fibrinogen. The supernatant is collected by centrifugation in a refrigerated centrifuge at 4°C. The supernatant is discarded and the precipitate is dissolved in buffer. This is then clotted with Thrombin and the time to clot lysis determined by inspection every 15 minutes.
A control plasma sample collected at the same time as the patient sample must be run in parallel.
The image below illustrates an ECLT:
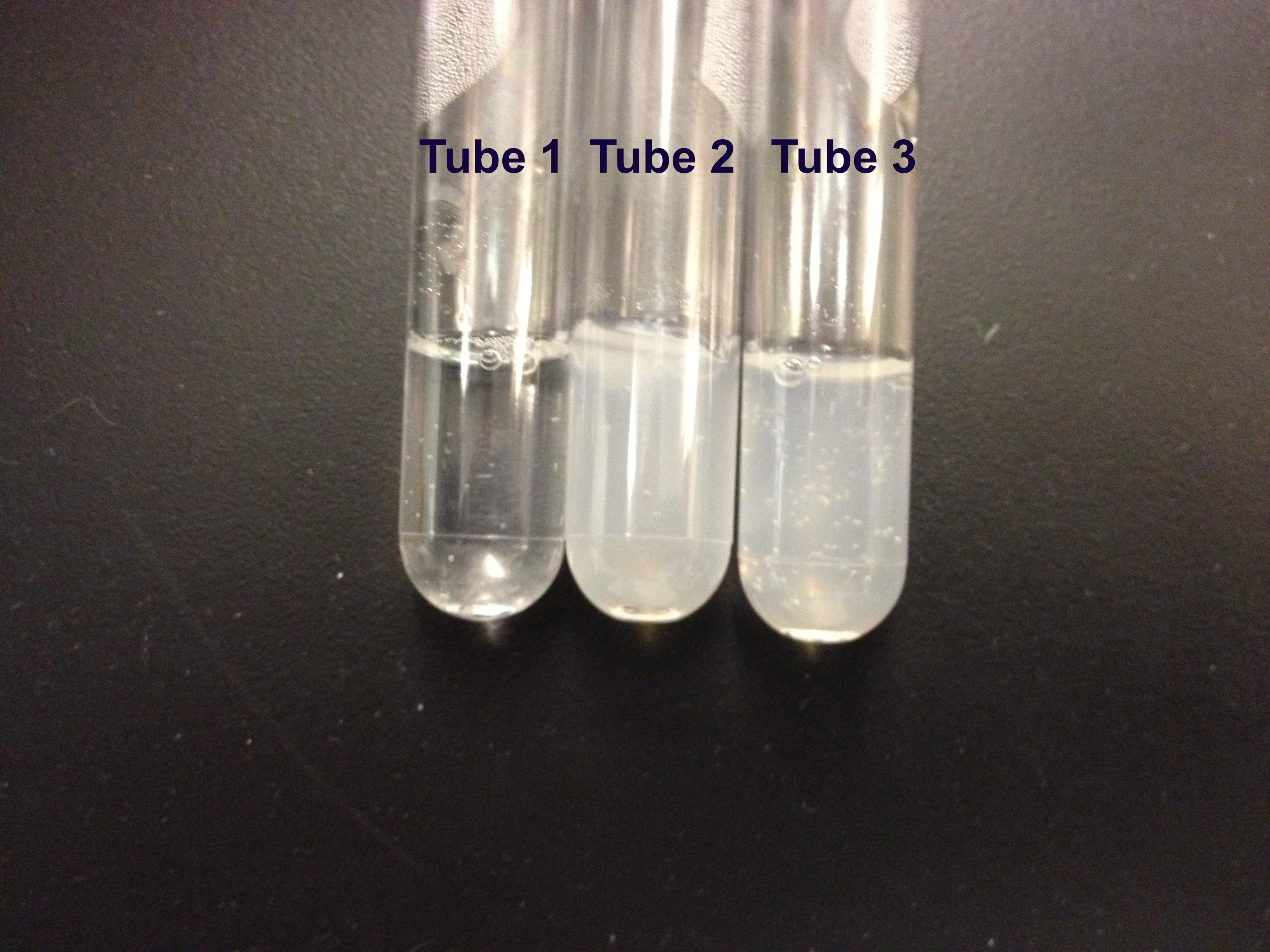
Tubes 2 and 3 are controls and show no lysis whereas in Tube 1 there is obvious lysis indicating hyperfibrinolysis.
Fibrin Plate Lysis
A Fibrinogen solution is poured onto a Petri dish and clotted with Thrombin and Calcium Chloride to form fibrin 'lawns.' The Euglobulin fraction under test is carefully pipetted onto the fibrin lawn. The plates are incubated at 37°C . The Plasminogen in the lawn is converted into Plasmin which leads to lysis of the fibrin lawn. The diameter of the zones of lysis are proportional to the concentration of the Plasminogen activator in the Euglobulin fraction. By running controls in parallel, zones of lysis which are larger than the control demonstrate hyperfibrinolysis whilst zones which are smaller show hypofibrinolysis.
Interpretation
Abnormalities of fibrinolysis are common and can be both physiological and pathological:
| Increased Fibrinolysis [Decreased ECLT] | Decreased Fibrinolysis [Increased ECLT] | |
|---|---|---|
| Physiological | Normal diurnal variation Exercise Venous Occlusion |
Normal diurnal variation 3rd trimester of Pregnancy |
| Pathological | Factor XIII deficiency In association with thrombolytic therapy e.g. t-PA, Streptokinase Following treatment with DDAVP |
DIC Liver disease During the anhepatic phase of liver transplantation Post-operatively In association with obesity In many cases of recurrent venous thromboses the significance of which is unclear |
Reference Ranges
Reference Range: 90-240 minutes
Hyperfibrinolysis: <60 minutes
Hypofibrinolysis: >240 minutes
What Test Next
In individuals with an abnormal ECLT, it may be useful to undertake specific assays of the components of the Fibrinolytic pathway, to perform a TEG/ROTEM or to sequence the relevant genes.