Impedance Platelet Aggregometry
Platelets are fundamental to primary haemostasis and their varied functions can be investigated using a variety of methodologies. Platelet function testing is time consuming and prone to a wide-variety of problems due to pre-analytical variables. Whole Blood Impedance Aggregometry measures the change in electrical impedance between two electrodes
when platelet aggregation is induced by an agonist. The method is performed using whole blood and so eliminates the need to generate platelet rich plasma [PRP].
Before undertaking any tests of platelet function - consider:
| Variable | Interpretation |
|---|---|
| Clinical History & examination. | Some syndromes [e.g. Hermansky Pudlak syndrome, Cheddiak Higashi syndrome, Wiskott-Aldrich syndrome, Velocardiofacial Syndrome (VCFS), Noonan syndrome, MYH9-related disorders] are associated with abnormal platelet function and you may get some idea of the diagnosis from the history, the family history and examination. |
| Drug History | There are a large number of drugs and food substances that can interfere with platelet function. |
| Full Blood Count (FBC) and Blood Film | 1. Pseudo-thrombocytopaenia: Often due to cold reacting platelet agglutinins or to platelet satellitism. Approximately 0.1% of the healthy population show EDTA-induced Pseudo-thrombocytopaenia and it is important to exclude this before undertaking more extensive tests of platelet function. Similar findings have also been reported with the use of both citrate and heparin as anticoagulants. A blood film may identify platelet clumps and provide a clue to the diagnosis. 2. Mean Platelet Volume: [MPV – reference range 7-10fL]: The MPV is an often ignored parameter of the FBC but can provide important insights into the causes of a low platelet count. - It can also in some cases give a clue to the diagnosis e.g. the hereditary macrothrombocytopenias, Bernard Soulier Syndrome [BSS] - In individuals with an elevated MPV, an immunological-based platelet count may provide a more accurate and often significantly higher platelet count. - The MPV can be an indication of platelet turnover – an increased MPV indicating accelerated platelet clearance as in ITP or gestational thrombocytopaenia. - The MPV may be reduced in cases of Wiskott-Aldrich Syndrome and in some cases of bone marrow failure. 3. Blood Film and Platelet Morphology: An examination of the blood film and platelet morphology can be useful in both establishing a diagnosis of Pseudo-thrombocytopaenia but also in establishing a primary platelet problem e.g. Gray Platelet Syndrome. In some cases of thrombocytopaenia e.g. May Hegglin anomaly – the blood film may show the presence of Döhle bodies [light blue-gray, oval, basophilic, leukocyte inclusions located in the peripheral cytoplasm of neutrophils.] |
Principles of Impedance Aggregometry
Platelet aggregation testing measures the ability of various platelet agonists to induce in vitro activation and platelet-to-platelet activation. In Impedance Aggregometry two electrodes are immersed into the whole blood sample and the impedance between the two electrodes is measured following the addition of various agonists. The sensor wires are made of highly conductive copper which are silver-coated.
As the platelets agglutinate or aggregate on the electrodes in response to the various agonists, the electrical resistance between the wires increases and this change in impedance is recorded continuously.
The commercial Multiplate® Analyzer has five separate channels and each of the sample test cells contains two independent sensors allowing simultaneous measurement of multiple different whole blood samples or alternatively a single whole blood sample using a variety of different agonists. Each test cell requires 300µL of whole blood for the analysis.
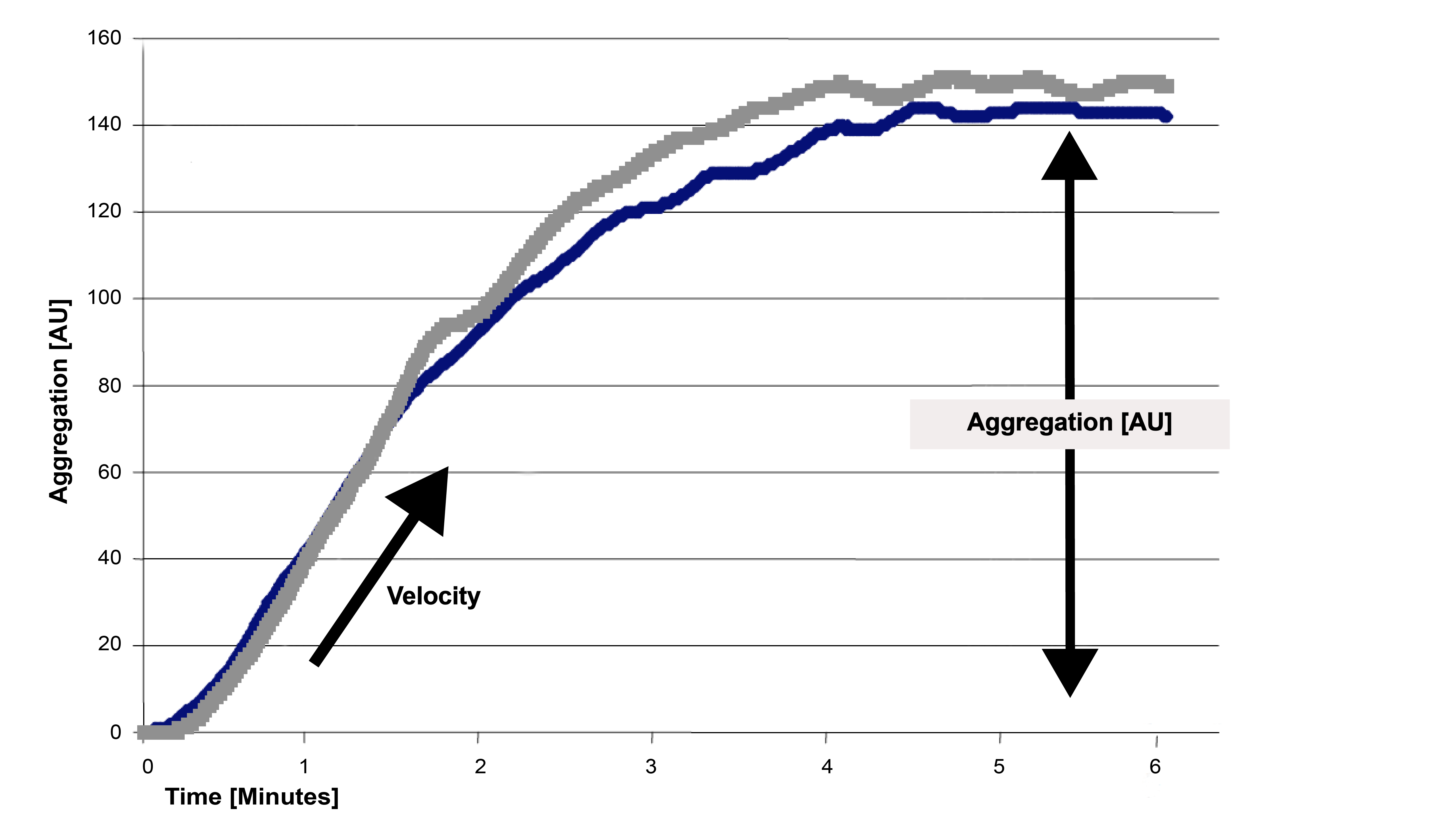
Three parameters are derived from each cell:
1. Aggregation - the height of the aggregation curve
2. Velocity - the maximum slope of the aggregation curve
3. Area Under the Curve [AUC] - reflects overall platelet activity, which is affected by the height of the aggregation curve
The Multiplate® Analyzer uses a number of agonists to investigate various aspects of platelet function:
| Test | Agonist: Concentration | |
|---|---|---|
| ADPtest | ADP: 200 µM | Induces platelet activation via the ADP receptors, releasing endogenous ADP and irreversible aggregation. Interaction of ADP with the P2Y1 receptor initiates the platelet response while interaction with the P2Y12 receptor promotes the response. Drugs [e.g. Clopidogrel, Prasugrel and Ticlopidine] or disorders of the P2Y12 receptor will lead to abnormal results. |
| ADPtest HS | ADP + PGE1: 200 µM + 300 nM | This test includes ADP and PGE1 [Prostaglandin E1]. PGE1 stimulates platelet adenyl cyclase activity, increasing cAMP concentration and which inhibits Ca2+ release and platelet aggregation induced by P2Y1 receptor activation. This increases the sensitivity of the test to samples containing Clopidogrel |
| ASPItest | Arachidonic Acid: 15 mM | Arachidonic Acid induces platelet activation which is inhibited by Aspirin. Arachidonic Acid is present in the granules and membranes of human platelets and and in the presence of the enzyme cyclooxygenase [COX-1], it generates the endoperoxide Prostaglandin G2 [PGG2]. PGG2 is quickly transformed to Prostaglandin H2 [PGH2] which in turn is converted to Thromboxane A2 [TxA2] - a potent inducer of platelet aggregation. Aspirin [and NSAIDs] inhibits the action of COX-1 and so prevents platelet activation. |
| COLtest | Collagen: 50 µg/mL | Collagen activates platelets by binding to platelet collagen receptors. The platelet has 3 main collagen receptors: α2β1, GpVI and vWF. Binding to all three receptors appears to be required for complete adhesion and activation of platelets. The COLtest is sensitive to the presence of Aspirin although less so that the ASPItest. |
| RISTOtest | Ristocetin RISTOlow 0.2 mg/mL RISTOhigh: 0.77 mg/mL |
Ristocetin binds to VWF leading to a conformational change in its structure that facilitates its binding to the platelet and subsequently its activation. The use of both high and low Ristocetin concentrations allows the identification of individuals with von Willebrands disease including Type 2B. |
| TRAPtest | TRAP-6 peptide: 1000 µM | Activates the platelet Thrombin Receptor using the Thrombin Receptor Activating Peptide [TRAP-6]. This pathway is not inhibited by Aspirin or Clopidogrel. It can be used to detect the action of GpIIb/IIIa antagonists. |
Interpretation
The interpretation of the data generated from Impedance Platelet Aggregometry [ Multiplate® Analyzer] is similar to that of Light Transmission Aggregometry. The Multiplate® Analyzer is increasingly used to monitor patients on anti-platelet drugs and in addition has been used to guide the timing of surgery in patients on anti-platelet drugs following their discontinuation.